Hip Flexors
Hip Flexors
Hip Flexors
Introduction

A hip flexor muscle is a muscle that functions in flexing the hip, ie bringing the knee closer to the chest. Hip flexion is maximal with a high, forward kick that brings the leg above the level of the waist[1]. Every time you take a step, you are using your hip flexor muscles.
- They are important to keep the posterior pelvic muscles in balance.
- Having a strong core is one way to strengthen hip flexors (along with practicing good posture).
- Stretching these muscles will also increase their length and help prevent injury[2].
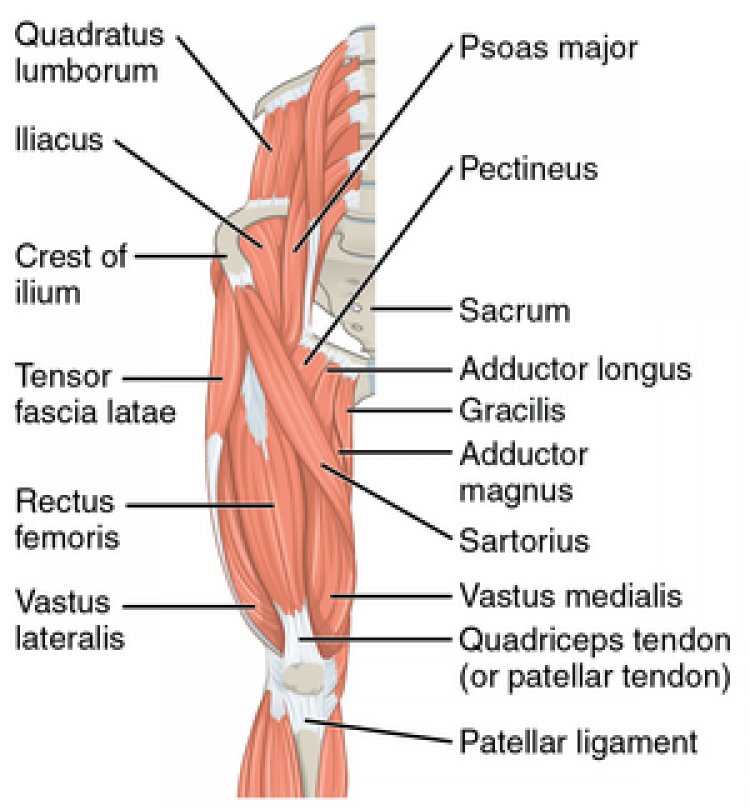
The hip flexors consist of 5 key muscles that contribute to hip flexion: iliacus, psoas, pectineus, rectus femoris, and sartorius.[3]
Prime Movers

The prime movers (agonist) for hip flexion are the:
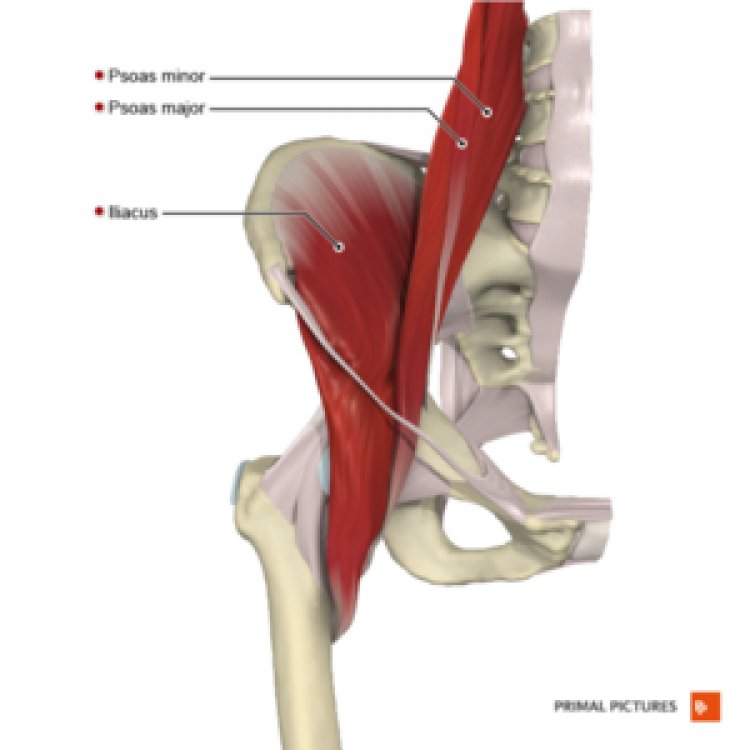
- Psoas major muscle, a long, tapering (fusiform) muscle that originates at either side of the spine and inserts at the lesser trochanter of the femur. The psoas muscle contracts when the hip is flexed. The psoas minor is a normal anatomic variant present in approximately 60% of people.
- Iliacus muscle. The iliacus muscle is a triangular sheet that connects the ilium bone to the lesser trochanter.

The iliacus and psoas muscles are often grouped together as the iliopsoas musculotendinous unit secondary to overlapping function and anatomic proximity. The iliopsoas has an associated bursa that is the largest bursa in the body and lies between the iliopsoas and the hip capsule/pubis.
- These 2 muscles contribute to postural stability while standing erect and elevating the torso from a supine position[3]. See also Functional Sequence of Balance Training Exercises
- The iliopsoas is the body’s most important hip flexor. People who spend the majority of the day sitting down have shorter hip flexor muscles, tilting the pelvis, and can change how the person walks. See Sitting Ergonomics And The Impact on Low Back Pain
Synergists

The rectus femoris is one of the quadriceps and a hip flexor muscle and has two functions: flex at the hip; extend the knee.[1]. Rectus Femoris is engaged intensely when both functions are at play, such as when kicking a soccer ball or swinging a straight leg forward.
The sartorius, the longest muscle in the body, crosses the hip and the knee joints. It originates at the anterior superior iliac spine and inserts superficially on the pes anserinus as a broad fascial insertion. It functions to flex the hip, and secondarily to adduct the thigh and externally rotate the leg. Like with Rectus Femoris, great effort from Sartorius is required during a soccer kick, particularly when kicking across the body.[4]
The pectineus acts as a hip flexor and secondary adductor from its origin on the superior pubic ramus and insertion on the pectineal line of the femur[1].
Physiotherapy Relevance
Postural Issues

Sitting too long or all day shortens and tightens these the hip muscles. This condition is a common problem with with people who sit for many hours daily eg anyone sits at a desk for hours each day; bus drivers. Shortened muscles are unable to generate as much power as lengthened muscles, which can lead to functional problems.eg causes anterior pelvic tilt and a lumber hyperlordosis[2].

See also Principles of Biomechanics in Hip Flexion Contracture
Another hip flexor issue related is Lower Crossed Syndrome. In LCS there is overactivity and tightness of hip flexors and lumbar extensors. Along with this there is underactivity and weakness of the deep abdominal muscles on the ventral side and of the gluteus maximus and medius on the dorsal side.
Injuries

Athletic injuries to the hip flexors and iliopsoas have been described in populations across all levels of competitive sports. Estimates of hip flexor pathology ranges from 5% of injuries all the way to 28% of injuries among high-risk sport-specific groups. Although most of these injuries are successfully treated with conservative management, and high rates of return to play are observed, significant rehabilitation time can be involved.[3]
Poor posture, general overuse, and sometimes arthritis can also cause pain in the hip flexors.[2]
- Strains, tears, tendinosis, and bursitis of the iliopsoas muscle can all present similarly.
- Overuse or eccentric hip flexion against resistance is often the cause.
- Bursitis or tendinosis is caused by overuse of the iliopsoas tendon resulting in friction as the tendon glides over the iliopectineal eminence.

Symptoms of an iliopsoas strain or tear are typically:
- groin and/or proximal medial thigh pain, which are exacerbated by actively flexing the hip against resistance
- pain with passive extension of the hip by stretching the iliopsoas tendon
- tenderness over the femoral triangle
- swelling may also be palpated.
Image 7: A potential hip injury move
Image 8: There is hardly a dancer who has never had some hip pain at some point.